Early Post-partum Recovery
International Journal of Childbirth Education. September 2009.
Heather Jeffcoat, DPT
After birth, the first six weeks are a critical period to begin exercise to get your body into pre-pregnancy shape. But, where to begin? Many changes occur in the musculoskeletal system during pregnancy and birth. The hormone Relaxin has influenced every joint in your client's body, creating ligamentous laxity which will last for 3-4 months post-delivery. This effect is longer if your client is breastfeeding. Their center of gravity is suddenly shifted, which can create problems with balance.
The abdominal muscles become gradually overstretched and weak with pregnancy. The hip flexor and lower back muscles tighten as they are placed in a shortened position due to postural changes that occur during pregnancy. Additionally, the pelvic floor muscles are stretched relatively quickly during vaginal birth, and tearing may occur. Unfortunately, these muscles do not immediately return to their pre-pregnancy states.
It is quite tempting to jump back into a rigorous exercise routine after birth, however due to all these changes, there are recommended exercise progressions for the early post-partum period. These recommendations are intended for women after a normal vaginal birth without complications during the post-partum period. If additional health concerns are present, consultation with a physician or midwife is advised prior to beginning any exercise program.
When muscles are overstretched, they develop what is called a "stretch weakness". This means that there is not adequate overlap of the muscle fibers to perform at an optimal level. This may lead to pain or dysfunction in this area. When this stretch weakness occurs in the abdominal muscles, there is the potential for developing lower back, pelvic or hip pain. In the pelvic floor, this stretch weakness may present as incontinence, prolapse or both.
Performing deep abdominal contractions and Kegel exercises are essential during the first six weeks. They should be started within the first 24 hours to prevent muscle atrophy. Performing Kegels will also increase local circulation, assisting with the healing process.
Instruct your client to perform isolated pelvic floor muscle contractions (Kegels) as described below:
Sample Kegel Progression
- Week 1: Hold 1 second ("Quick Flick"). Perform 2 sets of 5, 3 times per day.
- Week 2: Increase to 2 sets of 10, 2 times per day.
- Week 3: Increase to 2 sets of 15, 1 time per day.
- Week 4: Continue with Week 3 Routine, add 3 second holds ("Long Holds"), 2 sets of 5.
Continue to increase 3 second holds per Week 2 & 3 protocol. Once, up to 2 sets of 15, increase hold times to 5 seconds and reduce repetitions to 2 sets of 5 again. Continue to gradually increase repetitions. Your client's goal will be to perform "Long Holds" for 10 seconds, at least 2 sets of 10 daily
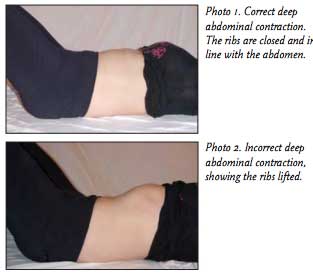
Deep abdominal contractions (Transverse Abdominus contractions) are also essential. Have your client lie on their back with their knees bent and with a natural curve in their lower back (neutral spine position). Instruct your client to gently pull their navel towards their spine (Photo 1). Breathing during this exercise should not be forced, and the contraction should be held at about a 30% effort. A common error to performing this exercise is shown in Photo 2. Instruct your client to begin with holding for 1 minute at a time, and increasing the hold time as they feel stronger.
As soon as possible, encourage your client to perform Kegels and deep abdominal muscle contractions simultaneously. These exercises should also be incorporated into daily activities, such as picking up their baby or squatting to the floor.
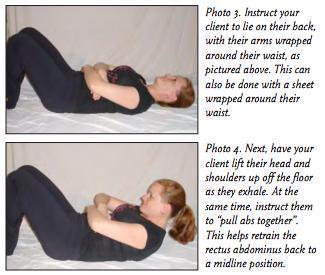
If a diastasis is present, this should be corrected to restore a more midline position of the rectus abdominus muscles (Photos 3 and 4). This separation should be reduced to two finger-widths before additional exercises are performed. This exercise should be performed two times per day for optimal results, 10 repetitions at a time to start. In a week, your client can begin to work up to 20 repetitions at a time.

Restoring pre-pregnancy flexibility is also important. The hip flexor and lower back muscles are especially susceptible as the growing abdomen pulls the pelvis anteriorly during pregnancy, creating shortness in these muscle groups (Photos 5 and 6). Two repetitions of each stretch should be performed and held for 30 seconds each. They should be repeated two times per day.
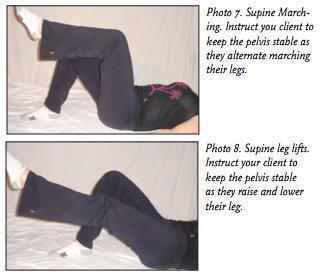
Additional exercises can be performed that help retrain the core muscles, even though the diastasis may be still present. These exercises should be performed daily, beginning with 8-10 repetitions and building up as your client's strength improves. These exercises should all be performed while maintaining a neutral position in the spine (Photos 7 and 8).
Crunches and oblique abdominal exercises should not be performed until the diastasis is corrected to two finger-widths or less. Once the diastasis is reduced to this amount, Pilates is an excellent way to further challenge the core muscles after pregnancy. Finally, your client should be encouraged to participate in a walking program, as it is a great way for them to resume their cardiovascular routine and burn the extra "baby fat". It is generally recommended to avoid running immediately post-partum. I recommend waiting during the first 6 weeks, as both the abdominal and pelvic floor muscles are generally too weak to adequately support this activity.
Of course, there may be factors that are present your clients did not anticipate. These may include back pain, incontinence or pelvic pain. Depending on your client's prior level of fitness or additional health considerations, the information provided above may need modification. Referral to a Women's Health physical therapist is indicated. If you don't know of one in your area, you can contact the American Physical Therapy Association's Section of Women's Health at
References
ACOG, 2005. Your pregnancy and birth. Washington, DC: Meredith Books.
Charteris, J., Goslin, B.R. In vivo approximations of the classic in vitro length-tension relationship: an isokinetic evaluation. Journal of Orthopaedic & Sports Physical Therapy. 1986 Mar; 7(5):222-231.
Cramer, J.T., et al. Acute effects of static stretching on peak torque in women. Journal of Strength and Conditioning Research. 2004; 18(2):236-241.
Noble, E. 1995. Essential exercises for the childbearing year. Harwich, MA: New Life Images.
Stephenson, R., O'Connor, L. 2000. Obstetric and Gynecologic Care in Physical Therapy. New Jersey: Slack, Inc.